
Royal College of Ophthalmologists | RCOphth
- admin
-
 Offline
Offline
- Posts: 1164
- Thanks: 153
Replied by admin on topic More about the RCO Refractive Surgery Standards...
Posted 09 Apr 2017 18:23 #21
This photo was taken in the lobby of the College at my first LAG meeting in April 2015, and I must have been crazy to seriously believe that I would ever be allowed any part in writing the standards!

Apart from any other reason, look at some of the College ‘Friends’ who’ve made financial contributions!
These include AMO, Alcon, Topcon, and Carl Zeiss. All major stakeholders in the refractive eye surgery industry worldwide, and definitely no fans of mine!
Before I return to my critique of the ‘NEW Refractive Surgery Standards and patient information improve quality of care and help patients make informed choices’, I recommend that you read the replies from the RSSWG in response to comments on the RCO consultation draft standards and patient information documents in 2016.
www.rcophth.ac.uk/wp-content/uploads/201...ne-2016-Comments.pdf
This is a small selection, and while I have made notes after some of the comments the rest should be self explanatory to anyone left with problems after refractive eye surgery!
• Page 3
RSSWG: 'We informed a range of stakeholders about the consultation including College Members, professional bodies, and employers of refractive surgeons. The consultation was advertised on the College website and we also issued a notification to the UK and Ireland Society of Cataract and Refractive Surgeons'
[The College was strongly criticised by campaigners and patients for the absence of information provided to the general public concerning the consultation, which we learned about at a late date only thanks to someone sending me an anonymous email. And, at a meeting on 12 October 2016, Shadow Chancellor John McDonnell advised the College that they should provide such information to me to post on my social media sites in future. The College have chosen not to do so.]
• Page 6
Optometrist: 'The use of the term "over 95%” satisfied is misleading as it is too subjective and undefined. It does not explain why 5% are not. "Side effects” implies temporary mild symptoms. This is untrue and is a minimising term. Better would be "serious and sometimes permanent life changing side effects”.
RSSWG reply: '95% is derived from validated questionnaire data referenced (e.g. Solomon KD et al Ophthalmology 2009 1). But the essential aim is indeed to target the up to 5% of patients who are not either satisfied or very satisfied with their outcome.
[I have no idea what the aim to ‘target the up to 5%’ means! Target for what?]
'Side effects are, by definition, self-limiting in the vast majority of cases. The current wording reflects the evidence base.'
[Self limiting definition: ultimately resolving itself without treatment.]
• Page 15
RSSWG: 'We acknowledge that more work needs to be done with patient reported outcome measures of vision quality, satisfaction with surgery, and other quality of life measures but some good evidence (cited) already exists’ [QED]
• Page 16
RSSWG: ‘Symptoms are usually minor and temporary. Untreatable, lasting problems resulting from surgery are rare. Although new eye discomfort symptoms occur in some patients after surgery, the majority (including ex contact lens wearers) are more comfortable.
• Page 17/18
Patient: 'As a laser eye surgery victim, I am very concerned by the new refractive surgery standards, as I cannot see how they will protect the public. I can see no warning of the constant pain that a potential patient could be left with for the rest of their life and the terrible psychological damage, that no amount of counselling etc. can cure, such as depression and in some cases suicide. I did not think that surgery would leave me with terrible RSSS, including PTSD, nor did I imagine that I would suffer unbearable physical pain for the rest of my life… People need to know that they may have to get out of bed every night for the rest of their lives, just to nurse their eyes, and they may not be able to drive at night etc. Their lives could be ruined, they may not be able to work.'
RSSWG reply: 'This level of negative impact is rare but very distressing. There is often (but not always) effective treatment for complications resulting from surgery and improving access is a priority. One of the important dimensions of our work in the RSSWG later this year will be to look at ways of enhancing support for patients with problems after surgery.’
[Sit in my chair for a few days and you'll find this level of negative impact is far from rare!]
• Page 20
RSSWG: “Your surgeon will advise you when it is safe to start driving again. Typically, this is within a few days of surgery”
[And the many 1,000s left unable to drive at night, if at all?]
• Page 26
RSSWG: ‘Feedback from elsewhere has been very positive. Illustrations and videos will be added once the text is finalised to help make the information as accessible as possible.’
[Positive feedback from where? And no videos or illustrations in the new standards - unsurprisingly, as who would risk it if they knew what could and too frequently does happen!]
• Page 27
College of Optometrists: 'We should be happy to ask our public patient reference group to comment on these documents if that is helpful.’
RSSWG reply: ‘The documents have been developed with feedback from the College lay advisory group and public consultation. We will set in place a mechanism for periodic revision but we are not planning any further consultation before the first release of the finalised documents’
[(i) Input from the Lay Advisory Group is akin to me sitting on a panel to give an opinion on standards for brain surgery!
(ii) Only three comments from patients included in the response doc, with no reference to patients’ input at the public consultation - six of us present
(iii) I complained to the College that nor was my written response included, and the College replied they didn’t realise I wanted it to be.]
• Page 33/34
RSSWG: 'We would like to see data on refractive surgery collected and reported on at a national level with the aim of deriving and presenting accurate contemporary outcome figures in an accurate, balanced and digestible form.’
[Until such time the 95% satisfaction statistic is inappropriate and unpalatable]
• Page 37
RSSWG: 'Lay feedback we have on readability is generally very positive.'
[From whom?]
• Page 47
RSSWG: 'The one week cooling off period is a compromise between CSIC guidance (2 weeks strongly supported by the RCOphth Lay Advisory and Professional Standards Groups)…’
[What about My Beautiful Eyes campaigners and damaged patients?]
The College claim, "The RSSWG collaborated and consulted widely with patients…”
I will be asking the College to provide evidence and data to support their claim
Apart from any other reason, look at some of the College ‘Friends’ who’ve made financial contributions!
These include AMO, Alcon, Topcon, and Carl Zeiss. All major stakeholders in the refractive eye surgery industry worldwide, and definitely no fans of mine!
Before I return to my critique of the ‘NEW Refractive Surgery Standards and patient information improve quality of care and help patients make informed choices’, I recommend that you read the replies from the RSSWG in response to comments on the RCO consultation draft standards and patient information documents in 2016.
www.rcophth.ac.uk/wp-content/uploads/201...ne-2016-Comments.pdf
This is a small selection, and while I have made notes after some of the comments the rest should be self explanatory to anyone left with problems after refractive eye surgery!
• Page 3
RSSWG: 'We informed a range of stakeholders about the consultation including College Members, professional bodies, and employers of refractive surgeons. The consultation was advertised on the College website and we also issued a notification to the UK and Ireland Society of Cataract and Refractive Surgeons'
[The College was strongly criticised by campaigners and patients for the absence of information provided to the general public concerning the consultation, which we learned about at a late date only thanks to someone sending me an anonymous email. And, at a meeting on 12 October 2016, Shadow Chancellor John McDonnell advised the College that they should provide such information to me to post on my social media sites in future. The College have chosen not to do so.]
• Page 6
Optometrist: 'The use of the term "over 95%” satisfied is misleading as it is too subjective and undefined. It does not explain why 5% are not. "Side effects” implies temporary mild symptoms. This is untrue and is a minimising term. Better would be "serious and sometimes permanent life changing side effects”.
RSSWG reply: '95% is derived from validated questionnaire data referenced (e.g. Solomon KD et al Ophthalmology 2009 1). But the essential aim is indeed to target the up to 5% of patients who are not either satisfied or very satisfied with their outcome.
[I have no idea what the aim to ‘target the up to 5%’ means! Target for what?]
'Side effects are, by definition, self-limiting in the vast majority of cases. The current wording reflects the evidence base.'
[Self limiting definition: ultimately resolving itself without treatment.]
• Page 15
RSSWG: 'We acknowledge that more work needs to be done with patient reported outcome measures of vision quality, satisfaction with surgery, and other quality of life measures but some good evidence (cited) already exists’ [QED]
• Page 16
RSSWG: ‘Symptoms are usually minor and temporary. Untreatable, lasting problems resulting from surgery are rare. Although new eye discomfort symptoms occur in some patients after surgery, the majority (including ex contact lens wearers) are more comfortable.
• Page 17/18
Patient: 'As a laser eye surgery victim, I am very concerned by the new refractive surgery standards, as I cannot see how they will protect the public. I can see no warning of the constant pain that a potential patient could be left with for the rest of their life and the terrible psychological damage, that no amount of counselling etc. can cure, such as depression and in some cases suicide. I did not think that surgery would leave me with terrible RSSS, including PTSD, nor did I imagine that I would suffer unbearable physical pain for the rest of my life… People need to know that they may have to get out of bed every night for the rest of their lives, just to nurse their eyes, and they may not be able to drive at night etc. Their lives could be ruined, they may not be able to work.'
RSSWG reply: 'This level of negative impact is rare but very distressing. There is often (but not always) effective treatment for complications resulting from surgery and improving access is a priority. One of the important dimensions of our work in the RSSWG later this year will be to look at ways of enhancing support for patients with problems after surgery.’
[Sit in my chair for a few days and you'll find this level of negative impact is far from rare!]
• Page 20
RSSWG: “Your surgeon will advise you when it is safe to start driving again. Typically, this is within a few days of surgery”
[And the many 1,000s left unable to drive at night, if at all?]
• Page 26
RSSWG: ‘Feedback from elsewhere has been very positive. Illustrations and videos will be added once the text is finalised to help make the information as accessible as possible.’
[Positive feedback from where? And no videos or illustrations in the new standards - unsurprisingly, as who would risk it if they knew what could and too frequently does happen!]
• Page 27
College of Optometrists: 'We should be happy to ask our public patient reference group to comment on these documents if that is helpful.’
RSSWG reply: ‘The documents have been developed with feedback from the College lay advisory group and public consultation. We will set in place a mechanism for periodic revision but we are not planning any further consultation before the first release of the finalised documents’
[(i) Input from the Lay Advisory Group is akin to me sitting on a panel to give an opinion on standards for brain surgery!
(ii) Only three comments from patients included in the response doc, with no reference to patients’ input at the public consultation - six of us present
(iii) I complained to the College that nor was my written response included, and the College replied they didn’t realise I wanted it to be.]
• Page 33/34
RSSWG: 'We would like to see data on refractive surgery collected and reported on at a national level with the aim of deriving and presenting accurate contemporary outcome figures in an accurate, balanced and digestible form.’
[Until such time the 95% satisfaction statistic is inappropriate and unpalatable]
• Page 37
RSSWG: 'Lay feedback we have on readability is generally very positive.'
[From whom?]
• Page 47
RSSWG: 'The one week cooling off period is a compromise between CSIC guidance (2 weeks strongly supported by the RCOphth Lay Advisory and Professional Standards Groups)…’
[What about My Beautiful Eyes campaigners and damaged patients?]
The College claim, "The RSSWG collaborated and consulted widely with patients…”
I will be asking the College to provide evidence and data to support their claim
Last Edit:14 Apr 2017 14:16
by admin
Please Log in or Create an account to join the conversation.
- Douglas Fury
So when performing invasive surgery on peoples eyes, a 5% failure rate is an acceptable success rate?
So OE and other suppliers of eye surgery are happy with a MANIPULATED 95% patient satisfaction.
It's easy to manipulate figures to provide statistics to present a somewhat false impression to potential customers that all is good and safe with their products/services.
Maybe they should take a leaf out of Samsung's responsibility to customers when Samsung recently had problems with their Galaxy Note 7 Smartphone overheating and going on fire.
Did Samsung come out and say, well 95% of our customers are happy and don't have a problem?
No, Samsung stood up to the potential life changing damage that could be caused and after only 35 reported incidents, they recalled 2.5 MILLION of the phones manufactured.
I'm not an expert on maths, (but I am a damaged OE patient) and to me, 35 out of 2.5 million equates to a failure of 0.0014% of manufactured phones having a problem.
In other words 99.9986% out of the 2.5 million manufactured were OK.
Now that is a success rate and shows how to take potential disastrous and life changing situations and product/supply success rate seriously.
RCO, NHS Choices, CQC et all, stand up and SEE that this industry is dangerous to Joe Public who are only informed of the Good Stories!
So OE and other suppliers of eye surgery are happy with a MANIPULATED 95% patient satisfaction.
It's easy to manipulate figures to provide statistics to present a somewhat false impression to potential customers that all is good and safe with their products/services.
Maybe they should take a leaf out of Samsung's responsibility to customers when Samsung recently had problems with their Galaxy Note 7 Smartphone overheating and going on fire.
Did Samsung come out and say, well 95% of our customers are happy and don't have a problem?
No, Samsung stood up to the potential life changing damage that could be caused and after only 35 reported incidents, they recalled 2.5 MILLION of the phones manufactured.
I'm not an expert on maths, (but I am a damaged OE patient) and to me, 35 out of 2.5 million equates to a failure of 0.0014% of manufactured phones having a problem.
In other words 99.9986% out of the 2.5 million manufactured were OK.
Now that is a success rate and shows how to take potential disastrous and life changing situations and product/supply success rate seriously.
RCO, NHS Choices, CQC et all, stand up and SEE that this industry is dangerous to Joe Public who are only informed of the Good Stories!
Last Edit:07 Apr 2017 16:15
by Douglas Fury
Please Log in or Create an account to join the conversation.
- admin
-
Offline
- Posts: 1164
- Thanks: 153
My main criticism of the 'New Refractive Surgery Standards' is the much repeated plug that ‘Over 95% of patients are satisfied with the outcome of surgery’.
This claim has been vehemently argued by campaigners throughout the entire farcical process, because although prospective patients are unlikely to go to the RCO website (did you?), this statistic will be repeated in every news article and advertorial about refractive surgery, published on NHS Choices, CQC website, and elsewhere!
Last year, arguing my concerns with a RSSWG panel member, he told me that 95% referred to the 'high end’ of the market. I replied that I could accept this for the 'high end’ providers (still 1 in 20 not satisfied), but, as OE allegedly undertake 60% of all refractive surgery performed in the UK, then this is wholly unacceptable across the board, and 100% untrue.
On 9 November 2016 I wrote to the RSSWG chair, Bruce Allan, and asked,
‘Dear Bruce
Please can you provide the following information.
Re UK per annum:
1. How many laser eye surgery operations are performed
2. How many of these are lasik and how many lasek
3. How many lens exchange operations are performed
4. How many of these are monofocal and how many multifocal
I look forward to your response.
Best wishes,
Sasha'
He didn’t reply...
Two days later I wrote again,
'Dear Bruce,
I assume that you did not receive my previous email as I've had no acknowledgement from you as yet.
You will of course have the stats I’ve requested at hand given the 95% success rate claimed by the RSSWG.
I therefore look forward to your earliest reply.
Best wishes,
Sasha'
Bruce replied,

'Dear Sasha
Please direct all future email enquiries relating to RSSWG outputs to the College. We do not have accurate contemporary figures for the numbers of refractive surgery procedures performed in the UK. This is one of the reasons that we would like to develop a National Outcomes Database in refractive surgery as discussed at the last patient engagement day. The 95% satisfaction figure holds up across the board in contemporary refractive surgery publications however, and may be conservative. Have a look at the source references for the standardised patient information documents for more information.
yours sincerely
Bruce Allan'
(Link to ‘source references’ www.rcophth.ac.uk/wp-content/uploads/201...ation-References.pdf )
Now I put as much trust in peer reviews as I do in multiple choice questionnaires (that’s another story), which is, not a lot!
To simplify my issue with peer reviews, imagine if someone were selling the same product as you: they publish rave reviews based on their positive (cherry picked) research data, but even though a competitor, you are hardly likely to criticise their publication, or refer to any of the existing negative research data, because by doing so you would be damaging your own sales! Therefore you approve the reviews.
Look at the ‘source refs’ to understand my concern, with authors including Jan Venter, Bruce Allan, Steve Schallhorn, Paul Rosen, Vincenzo Maurino, Dan Reinstein - and although you may not recognise some of the names, anyone who's had problems with OE will certainly be horrified to find Tweedledum (aka Stephen Hannan) included as co-author for a study on ‘Visual outcomes and patient satisfaction’.
If it weren’t so tragic it would be hysterically funny given the numbers of DISsatisfied patients Tweedles has replied to!
So that brings me to the crux of my argument!
Bruce Allan wrote, 'We do not have accurate contemporary figures for the numbers of refractive surgery procedures performed in the UK.’
Would someone please tell me if I am missing something, because I do not accept that you can quote ‘Over 95%’ when there is no number to apply it to!
'1.3. Summary Data supporting all claims and statements must be available for independent verification'
www.rcophth.ac.uk/wp-content/uploads/201...ndards-April2017.pdf
It seems the College are breaking their own guidelines!
This is also of concern,
'Ask your surgeon what the most common complications have been in their experience for this procedure, how often these have occurred and what the surgeon did to correct them. Consider how you would cope if anything went wrong’
Can you imagine any surgeon ever admitting the truth, including the fact that he’s being sued by a dozen patients or more whose eyes are IRREPARABLY damaged, and that irreparable mean there is NO FIX!
Or that in fact dry eyes are a chronic condition with no cure at 6 months post op, as OE surgeon Jonathan Carr recently told an unhappy and dissatisfied patient!
Another damaged patient wrote to me, ‘Left with vision problems after my first lasik ops, a second to correct the problems didn’t work at all. An independent surgeon I went to for an opinion told me "These types of operations are very good if done right first time, but very difficult or impossible to fix if not."'
This doesn't sit well either!
'As the RCOphth advocates statutory regulation for refractive surgery as a long-term solution’
www.rcophth.ac.uk/patients/refractive-surgery/
If that were the case why did Carrie MacEwen not use her position as College president any time during the last three years and meet wth Health Secretary Jeremy Hunt to discuss this? Why did she never ask to meet with Shadow Chancellor John McDonnell and offer her support for our campaign?
Carrie has vocally supported so many other eye health issues, with interviews to press and radio, yet not one word about refractive eye surgery!
I was on the Lay Advisory Group for nine months, sitting at the same table as Carrie MacEwen, and, other than at the last meeting I attended, not once did I hear Carrie - or any other lay member - so much as mention refractive eye surgery!
It was only at my final meeting on 28 January 2016 that the topic came up, when the lay members were asked to comment on the RSSWG drafts.
They didn’t have a clue what they were talking about (none had EVER shown any interest in my area of expertise yet expected me to contribute to theirs) with one member suggesting that operations shouldn't be conducted in silence.
Yup, that would really help stop people’s eyes being damaged!
When I was asked for my comment on the draft they didn’t actually want to hear what I had to say, and it was then that I finally decided there was no point in wasting any more of my time. The College had made it abundantly clear that the interests of their refractive surgeon members took precedence over damaged patients, and so I told Carrie MacEwen and RCO Hon Secretary Bill Newman (at the meeting to ‘handle’ me) what I thought about the entire farcical process. Then I gave them (and the industry) exactly what they had been hoping for, and quit!
However, the minutes of that meeting certainly did not reflect the circumstances of my resignation!
I quote,
‘Ms Rodoy had felt unable to adhere to the working protocols of the College and tendered her resignation. At the invitation of the Chairman the Group as whether or not to accept her resignation, the Members unanimously agreed to accept it.'
I laughed out loud when they took a vote on whether to accept my resignation, but certainly not surprised when all hands went up, because from day one it was patently obvious that I was a cuckoo in a nest of sycophants!
I have plenty more comments to make on the standards and will do so in due course, including the fact that they are unenforceable and Optical Express have made it clear that they have no intention of following them!
Meanwhile, can I suggest that all damaged patients, if you can, try to imagine you haven’t had surgery, read through the standards, and see if there is anything in them that would actually alert you to the fact that there's a real possibility that your eyes could end up as they have, without any chance of repair!
PS: Bizarrely, the RCO have tweeted to journalist Stuart Heritage following my criticism of his irresponsible blog on 3 April (see General Chat).


I wonder why they only refer to laser and don't mention lens exchange
This claim has been vehemently argued by campaigners throughout the entire farcical process, because although prospective patients are unlikely to go to the RCO website (did you?), this statistic will be repeated in every news article and advertorial about refractive surgery, published on NHS Choices, CQC website, and elsewhere!
Last year, arguing my concerns with a RSSWG panel member, he told me that 95% referred to the 'high end’ of the market. I replied that I could accept this for the 'high end’ providers (still 1 in 20 not satisfied), but, as OE allegedly undertake 60% of all refractive surgery performed in the UK, then this is wholly unacceptable across the board, and 100% untrue.
On 9 November 2016 I wrote to the RSSWG chair, Bruce Allan, and asked,
‘Dear Bruce
Please can you provide the following information.
Re UK per annum:
1. How many laser eye surgery operations are performed
2. How many of these are lasik and how many lasek
3. How many lens exchange operations are performed
4. How many of these are monofocal and how many multifocal
I look forward to your response.
Best wishes,
Sasha'
He didn’t reply...
Two days later I wrote again,
'Dear Bruce,
I assume that you did not receive my previous email as I've had no acknowledgement from you as yet.
You will of course have the stats I’ve requested at hand given the 95% success rate claimed by the RSSWG.
I therefore look forward to your earliest reply.
Best wishes,
Sasha'
Bruce replied,
'Dear Sasha
Please direct all future email enquiries relating to RSSWG outputs to the College. We do not have accurate contemporary figures for the numbers of refractive surgery procedures performed in the UK. This is one of the reasons that we would like to develop a National Outcomes Database in refractive surgery as discussed at the last patient engagement day. The 95% satisfaction figure holds up across the board in contemporary refractive surgery publications however, and may be conservative. Have a look at the source references for the standardised patient information documents for more information.
yours sincerely
Bruce Allan'
(Link to ‘source references’ www.rcophth.ac.uk/wp-content/uploads/201...ation-References.pdf )
Now I put as much trust in peer reviews as I do in multiple choice questionnaires (that’s another story), which is, not a lot!
To simplify my issue with peer reviews, imagine if someone were selling the same product as you: they publish rave reviews based on their positive (cherry picked) research data, but even though a competitor, you are hardly likely to criticise their publication, or refer to any of the existing negative research data, because by doing so you would be damaging your own sales! Therefore you approve the reviews.
Look at the ‘source refs’ to understand my concern, with authors including Jan Venter, Bruce Allan, Steve Schallhorn, Paul Rosen, Vincenzo Maurino, Dan Reinstein - and although you may not recognise some of the names, anyone who's had problems with OE will certainly be horrified to find Tweedledum (aka Stephen Hannan) included as co-author for a study on ‘Visual outcomes and patient satisfaction’.
If it weren’t so tragic it would be hysterically funny given the numbers of DISsatisfied patients Tweedles has replied to!
So that brings me to the crux of my argument!
Bruce Allan wrote, 'We do not have accurate contemporary figures for the numbers of refractive surgery procedures performed in the UK.’
Would someone please tell me if I am missing something, because I do not accept that you can quote ‘Over 95%’ when there is no number to apply it to!
'1.3. Summary Data supporting all claims and statements must be available for independent verification'
www.rcophth.ac.uk/wp-content/uploads/201...ndards-April2017.pdf
It seems the College are breaking their own guidelines!
This is also of concern,
'Ask your surgeon what the most common complications have been in their experience for this procedure, how often these have occurred and what the surgeon did to correct them. Consider how you would cope if anything went wrong’
Can you imagine any surgeon ever admitting the truth, including the fact that he’s being sued by a dozen patients or more whose eyes are IRREPARABLY damaged, and that irreparable mean there is NO FIX!
Or that in fact dry eyes are a chronic condition with no cure at 6 months post op, as OE surgeon Jonathan Carr recently told an unhappy and dissatisfied patient!
Another damaged patient wrote to me, ‘Left with vision problems after my first lasik ops, a second to correct the problems didn’t work at all. An independent surgeon I went to for an opinion told me "These types of operations are very good if done right first time, but very difficult or impossible to fix if not."'
This doesn't sit well either!
'As the RCOphth advocates statutory regulation for refractive surgery as a long-term solution’
www.rcophth.ac.uk/patients/refractive-surgery/
If that were the case why did Carrie MacEwen not use her position as College president any time during the last three years and meet wth Health Secretary Jeremy Hunt to discuss this? Why did she never ask to meet with Shadow Chancellor John McDonnell and offer her support for our campaign?
Carrie has vocally supported so many other eye health issues, with interviews to press and radio, yet not one word about refractive eye surgery!
I was on the Lay Advisory Group for nine months, sitting at the same table as Carrie MacEwen, and, other than at the last meeting I attended, not once did I hear Carrie - or any other lay member - so much as mention refractive eye surgery!
It was only at my final meeting on 28 January 2016 that the topic came up, when the lay members were asked to comment on the RSSWG drafts.
They didn’t have a clue what they were talking about (none had EVER shown any interest in my area of expertise yet expected me to contribute to theirs) with one member suggesting that operations shouldn't be conducted in silence.
Yup, that would really help stop people’s eyes being damaged!
When I was asked for my comment on the draft they didn’t actually want to hear what I had to say, and it was then that I finally decided there was no point in wasting any more of my time. The College had made it abundantly clear that the interests of their refractive surgeon members took precedence over damaged patients, and so I told Carrie MacEwen and RCO Hon Secretary Bill Newman (at the meeting to ‘handle’ me) what I thought about the entire farcical process. Then I gave them (and the industry) exactly what they had been hoping for, and quit!
However, the minutes of that meeting certainly did not reflect the circumstances of my resignation!
I quote,
‘Ms Rodoy had felt unable to adhere to the working protocols of the College and tendered her resignation. At the invitation of the Chairman the Group as whether or not to accept her resignation, the Members unanimously agreed to accept it.'
I laughed out loud when they took a vote on whether to accept my resignation, but certainly not surprised when all hands went up, because from day one it was patently obvious that I was a cuckoo in a nest of sycophants!
I have plenty more comments to make on the standards and will do so in due course, including the fact that they are unenforceable and Optical Express have made it clear that they have no intention of following them!
Meanwhile, can I suggest that all damaged patients, if you can, try to imagine you haven’t had surgery, read through the standards, and see if there is anything in them that would actually alert you to the fact that there's a real possibility that your eyes could end up as they have, without any chance of repair!
PS: Bizarrely, the RCO have tweeted to journalist Stuart Heritage following my criticism of his irresponsible blog on 3 April (see General Chat).
I wonder why they only refer to laser and don't mention lens exchange
Last Edit:06 Apr 2017 18:48
by admin
Please Log in or Create an account to join the conversation.
- admin
-
Offline
- Posts: 1164
- Thanks: 153
RCO president Carrie MacEwan emailed Shadow Chancellor John McDonnell on Friday but chose not to copy me in, even though John had asked the College to inform me directly of any updates!
Carrie needs to put her dislike of me aside, because, no matter what she or her College cohorts think about me, I’m going nowhere, and unlike theirs, my priority is to safeguard patients not my income!
As she advised John, the ‘NEW Refractive Surgery Standards' are now online - and no better than we expected!
I have yet to read in depth, but this immediately jumped out at me, "The RSSWG collaborated and consulted widely with patients…”
Bullsh*t!
I will give you time to read the standards before publishing my response
www.rcophth.ac.uk/2017/04/new-refractive...tient-information-2/
Carrie needs to put her dislike of me aside, because, no matter what she or her College cohorts think about me, I’m going nowhere, and unlike theirs, my priority is to safeguard patients not my income!
As she advised John, the ‘NEW Refractive Surgery Standards' are now online - and no better than we expected!
I have yet to read in depth, but this immediately jumped out at me, "The RSSWG collaborated and consulted widely with patients…”
Bullsh*t!
I will give you time to read the standards before publishing my response
www.rcophth.ac.uk/2017/04/new-refractive...tient-information-2/
Last Edit:04 Apr 2017 10:10
by admin
Please Log in or Create an account to join the conversation.
- admin
-
Offline
- Posts: 1164
- Thanks: 153
We have to wait a little longer before we can ask health ministers to clarify exactly how the revised College standards (+CQC) will make the industry safe for patients as they have claimed (so no need for government regulation!).
Last Edit:02 Apr 2017 13:18
by admin
Please Log in or Create an account to join the conversation.
- admin
-
Offline
- Posts: 1164
- Thanks: 153
On 2 March, in response to my emailed query, Royal College of Ophthalmologists (RCO) Chief Executive Kathy Evans replied, "It remains our intention to publish the [Refractive Surgery] standards shortly and we are still working to a 31 March 2017 deadline.”
www.rcophth.ac.uk/standards-publications...e-surgery-standards/
That’s tomorrow!
As most of you know, David Teenan is OE's Medical Director and a core member of the Refractive Surgery Standards Working Group (RSSWG) responsible for updating the RCO guidelines/standards.
In addition, most input from damaged patients was condescendingly dismissed by the WG in their response to the farcical public consultation last May, a virtual secret until it was leaked to me the night before registration ended, so that at least some of us managed to attend!
Therefore, I promise you that the College revisions will do little or nothing to benefit future patients - and certainly nothing to help those of us already irreparably damaged by this unregulated industry.
With concerns for this industry expressed to the government as far back as 2004, a parliamentary panel was formed and their report published in 2005, with recommendations for the Royal College of Ophthalmologists, the College of Optometrists and the Healthcare Commission regarding "stricter standards of regulation for refractive surgery.” (John McDonnell MP was one of the panel and why I initially contacted him for support)
Its critics were notably refractive surgeons - unsurprisingly with strong links to Optical Express - and Emmanuel Rosen was one of these (whose younger cousin Paul was OE’s medicolegal expert in the Stephanie Holloway trial in 2014, criticised by Judge Bailey for not disclosing his conflict of interests as he had worked for Optical Express after the Rosen clinics were 'acquired' by OE)
www.opticalexpressgroup.com/optical-expr...osen-eye-clinic.html
'"As for future developments, a debate in parliament must occur before legislation is enacted, and according to Mr. [Emmanuel] Rosen, that could take some time… "That won't happen just like that because the legislation takes a long time in the U.K. and a long debate, and sometimes nothing is adopted, and sometimes some things are," he said.”'
www.healio.com/ophthalmology/news/print/...of-laser-eye-surgery
No sh*t Sherlock! Especially when you have a government seemingly as corrupt as the industry, who continue to refuse to acknowledge this major scandal, with health ministers having cancelled too many meetings with me since 2014 for it to be thought anything other than deliberate avoidance!!
A scandal that is not only damaging people’s eyes and lives, but also costing the NHS and the UK untold £millions, both in medical care and benefits claimed by those no longer able to work as a result of this unregulated surgery.
And with OE now adamant that aftercare will be refused to their customers beyond 12 months post op, no prizes for guessing who will pick up the pieces!
For those who may not realise just how serious an issue this is, imagine if you had an operation on the NHS; for example, something that left you unable to walk, still in need of medication and physio treatment 12 months later, but the hospital tells you, ‘Still in pain, can’t walk? Tough, your time’s up - suck it up and crawl!'
That's exactly what OE is doing, blatantly and unashamedly telling people that they won’t do anything more for them unless they pay - for OE to treat the problems they themselves caused!!
I've seen dozens of letters signed by Tweedledum (aka Stephen Hannan) that essentially tell damaged patients, 'We’ve had your money and we’re not going to waste any more of ours trying to fix you!"
And as more and more people discover this (keep in mind the 100s x 1,000s people OE claim to have operated on over the years) the NHS is going to be hard hit trying to help so many with nowhere else to turn!
But according to the health ministers that’s OK, as they regurgitate the same old mantra to MPs concerned for their suffering constituents, ’There is no problem, the RCO, GMC, and CQC have it under control’!
And don’t forget the 10s x £millions written off in taxes following the legal scam of putting clinics into administration while continuing to trade. And the government are OK with that too!
As a damaged patient, campaigner, and patient advocate, who's invested six years into researching its every corner, waded amidst its corruption, and so much more, even Russell Ambrose (Optimax) would agree that this industry is my specialist subject!
It unarguably made sense therefore that I should have been included in revising the RCO guidelines/standards. And the College thought so too, which is why they nominated and appointed me as lay advisor to the RSSWG on 7 May 2015.
At the time I was asked by the College not to publish details of my appointment because - according to the first lie they told me - they still hadn’t confirmed the surgeon members.
I learned the truth when the College removed me from the position almost eight weeks later, they had received complaints from David Moulsdale, and, wanting to keep him happy, were trying to figure out how to remove me without any noise. As if!
Most of you know the history, but for more recent OERML readers who missed it…
My subsequent SARs to David Moulsdale and the RCO disclosed collusion between both parties, including evidence of cosy Saturday afternoon chats between RSSWG chair, Moorfields surgeon Bruce Allan, and David Moulsdale - who, with the help of his legal team Schillings, was actually advising the College how to remove me from the RSSWG!!
In one email he told the College that five out of six of the surgeons on the panel were against my inclusion. And in case anyone is in doubt, David Moulsdale is the CEO of Optical Express, not a surgeon, and should therefore have had no part in decisions made by the RCO, nor should he have been party to this info. I have no doubt that David Teenan passed on this info and am aware David Moulsdale lobbied the other WG surgeons too.
When we attended what was no less than a rigged meeting with their hand picked trustees in December 2015, to argue for my reinstatement to the RSSWG, RCO trustee Peter Tiffin told Shadow Chancellor John McDonnell that they had to keep OE on board because they wouldn't agree to the standards otherwise.
John laughed out loud!
It was at this same meeting that the current RCO president Carrie MacEwan lied to both John and me when she said there was no point in reinstating me because the standards were almost finished and would be completed by the end of January 2016. She also lied that David Teenan was independent and didn't work for OE!
And as we all know, it’s now March 2017 and no standards published yet, and for the record, David Teenan works exclusively for OE and is their UK Medical Director, although I trust not for much longer given the numbers suing him - a fact the RCO knew but didn’t consider important btw!
www.pressreader.com/uk/the-herald/20160113/281573764690517
It doesn’t matter whether someone personally like or dislikes me, my value is in the experience and knowledge I have of this industry and the problems suffered by thousands of damaged patients I have personally spoken with.
So here’s a simple question for anyone who hasn’t considered it before: why would the College - purporting to be revising the standards/guidelines for the benefit of patients - not value my unique contribution, not least as a representative and spokesperson for damaged patients?
Here’s a clue, in 2009 the revised standards for laser refractive surgery clearly stated,
" a) Who the Standards are for:
These Standards are intended to assist medical, and other healthcare professionals involved in laser refractive surgery, as well as those involved in the administration of facilities where such surgery is performed"
www.rcophth.ac.uk/wp-content/uploads/201...andards-MAY-2009.pdf
If you are a laser patient damaged after 2009, and can be bothered reading the document, how much did these revisions help protect you? The answer is a resounding THEY DID NOT!
NB: The new revisions cover all refractive surgery, draft documents published last year:
www.rcophth.ac.uk/standards-publications...dards-consultations/
It should also be remembered that not only are the RCO guidelines totally unenforceable, but the majority of the surgeons responsible for the revisions are themselves refractive ophthalmologists who greatly profit from this unregulated industry!
Sniff sniff… can you smell that whiff of 'let’s protect our cash cow'
Meanwhile, I look forward to reading the long awaited revised RCO standards tomorrow, and then I’ll explain just why they aren't good enough!
www.rcophth.ac.uk/standards-publications...e-surgery-standards/
That’s tomorrow!
As most of you know, David Teenan is OE's Medical Director and a core member of the Refractive Surgery Standards Working Group (RSSWG) responsible for updating the RCO guidelines/standards.
In addition, most input from damaged patients was condescendingly dismissed by the WG in their response to the farcical public consultation last May, a virtual secret until it was leaked to me the night before registration ended, so that at least some of us managed to attend!
Therefore, I promise you that the College revisions will do little or nothing to benefit future patients - and certainly nothing to help those of us already irreparably damaged by this unregulated industry.
With concerns for this industry expressed to the government as far back as 2004, a parliamentary panel was formed and their report published in 2005, with recommendations for the Royal College of Ophthalmologists, the College of Optometrists and the Healthcare Commission regarding "stricter standards of regulation for refractive surgery.” (John McDonnell MP was one of the panel and why I initially contacted him for support)
Its critics were notably refractive surgeons - unsurprisingly with strong links to Optical Express - and Emmanuel Rosen was one of these (whose younger cousin Paul was OE’s medicolegal expert in the Stephanie Holloway trial in 2014, criticised by Judge Bailey for not disclosing his conflict of interests as he had worked for Optical Express after the Rosen clinics were 'acquired' by OE)
www.opticalexpressgroup.com/optical-expr...osen-eye-clinic.html
'"As for future developments, a debate in parliament must occur before legislation is enacted, and according to Mr. [Emmanuel] Rosen, that could take some time… "That won't happen just like that because the legislation takes a long time in the U.K. and a long debate, and sometimes nothing is adopted, and sometimes some things are," he said.”'
www.healio.com/ophthalmology/news/print/...of-laser-eye-surgery
No sh*t Sherlock! Especially when you have a government seemingly as corrupt as the industry, who continue to refuse to acknowledge this major scandal, with health ministers having cancelled too many meetings with me since 2014 for it to be thought anything other than deliberate avoidance!!
A scandal that is not only damaging people’s eyes and lives, but also costing the NHS and the UK untold £millions, both in medical care and benefits claimed by those no longer able to work as a result of this unregulated surgery.
And with OE now adamant that aftercare will be refused to their customers beyond 12 months post op, no prizes for guessing who will pick up the pieces!
For those who may not realise just how serious an issue this is, imagine if you had an operation on the NHS; for example, something that left you unable to walk, still in need of medication and physio treatment 12 months later, but the hospital tells you, ‘Still in pain, can’t walk? Tough, your time’s up - suck it up and crawl!'
That's exactly what OE is doing, blatantly and unashamedly telling people that they won’t do anything more for them unless they pay - for OE to treat the problems they themselves caused!!
I've seen dozens of letters signed by Tweedledum (aka Stephen Hannan) that essentially tell damaged patients, 'We’ve had your money and we’re not going to waste any more of ours trying to fix you!"
And as more and more people discover this (keep in mind the 100s x 1,000s people OE claim to have operated on over the years) the NHS is going to be hard hit trying to help so many with nowhere else to turn!
But according to the health ministers that’s OK, as they regurgitate the same old mantra to MPs concerned for their suffering constituents, ’There is no problem, the RCO, GMC, and CQC have it under control’!
And don’t forget the 10s x £millions written off in taxes following the legal scam of putting clinics into administration while continuing to trade. And the government are OK with that too!
As a damaged patient, campaigner, and patient advocate, who's invested six years into researching its every corner, waded amidst its corruption, and so much more, even Russell Ambrose (Optimax) would agree that this industry is my specialist subject!
It unarguably made sense therefore that I should have been included in revising the RCO guidelines/standards. And the College thought so too, which is why they nominated and appointed me as lay advisor to the RSSWG on 7 May 2015.
At the time I was asked by the College not to publish details of my appointment because - according to the first lie they told me - they still hadn’t confirmed the surgeon members.
I learned the truth when the College removed me from the position almost eight weeks later, they had received complaints from David Moulsdale, and, wanting to keep him happy, were trying to figure out how to remove me without any noise. As if!
Most of you know the history, but for more recent OERML readers who missed it…
My subsequent SARs to David Moulsdale and the RCO disclosed collusion between both parties, including evidence of cosy Saturday afternoon chats between RSSWG chair, Moorfields surgeon Bruce Allan, and David Moulsdale - who, with the help of his legal team Schillings, was actually advising the College how to remove me from the RSSWG!!
In one email he told the College that five out of six of the surgeons on the panel were against my inclusion. And in case anyone is in doubt, David Moulsdale is the CEO of Optical Express, not a surgeon, and should therefore have had no part in decisions made by the RCO, nor should he have been party to this info. I have no doubt that David Teenan passed on this info and am aware David Moulsdale lobbied the other WG surgeons too.
When we attended what was no less than a rigged meeting with their hand picked trustees in December 2015, to argue for my reinstatement to the RSSWG, RCO trustee Peter Tiffin told Shadow Chancellor John McDonnell that they had to keep OE on board because they wouldn't agree to the standards otherwise.
John laughed out loud!
It was at this same meeting that the current RCO president Carrie MacEwan lied to both John and me when she said there was no point in reinstating me because the standards were almost finished and would be completed by the end of January 2016. She also lied that David Teenan was independent and didn't work for OE!
And as we all know, it’s now March 2017 and no standards published yet, and for the record, David Teenan works exclusively for OE and is their UK Medical Director, although I trust not for much longer given the numbers suing him - a fact the RCO knew but didn’t consider important btw!
www.pressreader.com/uk/the-herald/20160113/281573764690517
It doesn’t matter whether someone personally like or dislikes me, my value is in the experience and knowledge I have of this industry and the problems suffered by thousands of damaged patients I have personally spoken with.
So here’s a simple question for anyone who hasn’t considered it before: why would the College - purporting to be revising the standards/guidelines for the benefit of patients - not value my unique contribution, not least as a representative and spokesperson for damaged patients?
Here’s a clue, in 2009 the revised standards for laser refractive surgery clearly stated,
" a) Who the Standards are for:
These Standards are intended to assist medical, and other healthcare professionals involved in laser refractive surgery, as well as those involved in the administration of facilities where such surgery is performed"
www.rcophth.ac.uk/wp-content/uploads/201...andards-MAY-2009.pdf
If you are a laser patient damaged after 2009, and can be bothered reading the document, how much did these revisions help protect you? The answer is a resounding THEY DID NOT!
NB: The new revisions cover all refractive surgery, draft documents published last year:
www.rcophth.ac.uk/standards-publications...dards-consultations/
It should also be remembered that not only are the RCO guidelines totally unenforceable, but the majority of the surgeons responsible for the revisions are themselves refractive ophthalmologists who greatly profit from this unregulated industry!
Sniff sniff… can you smell that whiff of 'let’s protect our cash cow'
Meanwhile, I look forward to reading the long awaited revised RCO standards tomorrow, and then I’ll explain just why they aren't good enough!
Last Edit:30 Mar 2017 22:34
by admin
Please Log in or Create an account to join the conversation.
- Disgusted
I do not believe that the new Guidelines to Standards for Laser Refractive Surgery will do even the slightest thing to protect the public. To add insult to injury, some ophthalmologists are now claiming to have been involved in the development of these guidelines to promote themselves, when in fact they were not members of the RCOphth Refractive Surgery Standards Working Group.
Advertising for St James Laser Vision, makes the claim that Andrew Morrell was "chosen among his peers to co-develop the Royal College Guidelines to Standards for Laser Refractive Surgery"
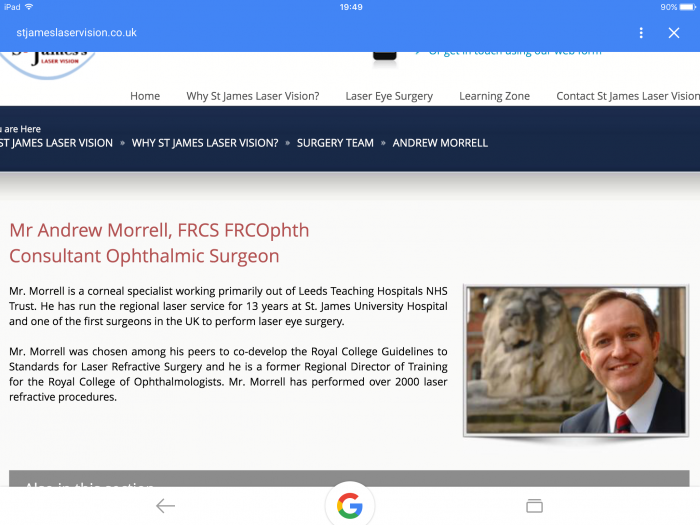
Anyone reading this could be excused for thinking that he was a member of the RCOphth Working Group - he is not. By misleading the public in this way surgeons like Andrew Morrell simply highlight that their industry is corrupt and only concerned with making money!
Advertising for St James Laser Vision, makes the claim that Andrew Morrell was "chosen among his peers to co-develop the Royal College Guidelines to Standards for Laser Refractive Surgery"
Anyone reading this could be excused for thinking that he was a member of the RCOphth Working Group - he is not. By misleading the public in this way surgeons like Andrew Morrell simply highlight that their industry is corrupt and only concerned with making money!
Last Edit:23 Feb 2017 17:45
by Disgusted
Please Log in or Create an account to join the conversation.
- Maria
John is a true advocate for reform in this industry.
I was at the meeting and what I found frustrating was how (as a damaged patient) I felt the RCO humoured me and my concerns. How else do they explain the lack of the voice of damaged patients in their working group? Industry politics I guess.
Thank you Sasha and John for your commitment to this cause. Many frustrations ahead I suspect…
I was at the meeting and what I found frustrating was how (as a damaged patient) I felt the RCO humoured me and my concerns. How else do they explain the lack of the voice of damaged patients in their working group? Industry politics I guess.
Thank you Sasha and John for your commitment to this cause. Many frustrations ahead I suspect…
Last Edit:07 Nov 2016 22:15
by Maria
Please Log in or Create an account to join the conversation.
- admin
-
Offline
- Posts: 1164
- Thanks: 153
Last week I met with Shadow Chancellor John McDonnell, for whom I have the greatest respect...
Although I can’t yet disclose the main purpose of our meeting, I can tell you that we also discussed Bernie Chang, the MHRA, the expected demise of Optical Express, and the meeting we attended at the Royal College of Ophthalmologists last month.
The RCO meeting was part of the College’s farcical consultation process re the new standards being written by the Refractive Surgery Standards Working Group, to discuss data collection and redress for damaged patients (see 12 October post). John had to leave before its end and he asked me to update him on what he’d missed.
I told him that I’d upset Bruce Allen (who chaired the meeting) when I vociferously argued against the College’s intent to publish an unsubstantiated 95% success rate in the new standards, which Bruce and his colleagues claim is supported by reliable data.
I asked Bruce, how can you rely on data provided (and omitted) by liars
If OE provide 60% of the market (Optimax/Ultralase approx 20%) then there is no way that the RCO can justifiably claim a 95% success rate. I accused Bruce of protecting his cash cow.
I also told him that I’d seen the emails he’d exchanged with David Moulsdale last year, conspiring to (successfully) remove me from my position as lay adviser on the Working Group. I swear I saw his hackles rise as he blustered and said I was free to share that info with my supporters if I wished. He presumably didn’t know that I did so last year! (September 2015 posts)
Bruce Allen wasn’t my biggest fan to start with, but I guess I'm definitely off his xmas card list now!
John asked me what I thought of Bruce's suggestion (re redress) that the industry contribute to an insurance scheme to compensate damaged patients. I told him this was nonsense, not least because who will decide if the patient has been left with problems!
I’ve read enough letters from Tweedles (aka Stephen Hannan) telling OE’s damaged patients that there’s nothing wrong with their eyes, while lawyers currently have a difficult enough job finding unbiased and honest medicolegal experts to write reports for patients lucky enough to be in litigation - ‘lucky' only because there are vast numbers of damaged patients unable to get legal representation for a myriad of reasons.
So an insurance scheme is a ridiculous and unworkable idea!
The College have proven their impotence, and their unwillingness to fight Optical Express - in fact kowtowing to them - and my biggest concern is that the College will publish a 95% success rate that will be quoted by the CQC, GMC, NHS, and included in every article written about eye surgery from then on.
Why would anyone but us damaged patients have reason to doubt statistics published by the Royal College of Opthalmologists!

Although I can’t yet disclose the main purpose of our meeting, I can tell you that we also discussed Bernie Chang, the MHRA, the expected demise of Optical Express, and the meeting we attended at the Royal College of Ophthalmologists last month.
The RCO meeting was part of the College’s farcical consultation process re the new standards being written by the Refractive Surgery Standards Working Group, to discuss data collection and redress for damaged patients (see 12 October post). John had to leave before its end and he asked me to update him on what he’d missed.
I told him that I’d upset Bruce Allen (who chaired the meeting) when I vociferously argued against the College’s intent to publish an unsubstantiated 95% success rate in the new standards, which Bruce and his colleagues claim is supported by reliable data.
I asked Bruce, how can you rely on data provided (and omitted) by liars
If OE provide 60% of the market (Optimax/Ultralase approx 20%) then there is no way that the RCO can justifiably claim a 95% success rate. I accused Bruce of protecting his cash cow.
I also told him that I’d seen the emails he’d exchanged with David Moulsdale last year, conspiring to (successfully) remove me from my position as lay adviser on the Working Group. I swear I saw his hackles rise as he blustered and said I was free to share that info with my supporters if I wished. He presumably didn’t know that I did so last year! (September 2015 posts)
Bruce Allen wasn’t my biggest fan to start with, but I guess I'm definitely off his xmas card list now!
John asked me what I thought of Bruce's suggestion (re redress) that the industry contribute to an insurance scheme to compensate damaged patients. I told him this was nonsense, not least because who will decide if the patient has been left with problems!
I’ve read enough letters from Tweedles (aka Stephen Hannan) telling OE’s damaged patients that there’s nothing wrong with their eyes, while lawyers currently have a difficult enough job finding unbiased and honest medicolegal experts to write reports for patients lucky enough to be in litigation - ‘lucky' only because there are vast numbers of damaged patients unable to get legal representation for a myriad of reasons.
So an insurance scheme is a ridiculous and unworkable idea!
The College have proven their impotence, and their unwillingness to fight Optical Express - in fact kowtowing to them - and my biggest concern is that the College will publish a 95% success rate that will be quoted by the CQC, GMC, NHS, and included in every article written about eye surgery from then on.
Why would anyone but us damaged patients have reason to doubt statistics published by the Royal College of Opthalmologists!
Last Edit:07 Nov 2016 23:12
by admin
Please Log in or Create an account to join the conversation.
- admin
-
Offline
- Posts: 1164
- Thanks: 153
Moderators: admin, Sasha